By Maya Doyle, Ashleigh Morris and Karishma Nanhu
This article is part of the National Trusts’ month-long tribute to commemorate the 175th anniversary of Indian Indentureship in Trinidad. Through a series of ongoing blog posts the Trust has explored the journey of the Indians to Trinidad on the Fath al Razack in 1845. This essay delves further into the topic of health and medical concerns as they pertain to Indian indentureship, an issue which the authorities who were managing the system claimed was important. The British colonial authorities claimed that emigration was advantageous to Indians. Indians were encouraged to leave India with promises of a better life in the West Indies. In reality it was an ordeal. From early on in the indentureship system it was recognized that the health of the emigrants before embarkation was a key feature affecting their chances of survival during the migration process. This article gives an introduction to some of the health concerns pertaining to the Indian indentureship system overall and in Trinidad.
At all points of the indenture system—the Emigration Depot, on ships, the Immigration Depot, the estates—medical provisions for labourers fell short. The ratio of doctors to patients, the amount of medicines and the numbers of beds for patients were insufficient. All of this was in the context of psychological stress as a result of homesickness, new experiences, the demanding life of plantation labour and the occupational hazards of the job. Arguably measures were continuously taken to alleviate conditions for indentured Indians but the pace of change was slow, based on trial and error, and it was always within the context of the Eurocentric opinion of Indians.
The quality of facilities provided for indentured Indians was influenced by British colonial perceptions of India, and what was adequate for Indians. As a result, overcrowding and poor hygiene contributed to the substandard sanitation throughout the system. This resulted in the prevalence of diseases which reduced labourers’ chances of survival, and their capacity to work.
The ideal Indian emigrant to Trinidad and other colonies was a young adult, capable of performing physically demanding agricultural labour who had a clean bill of health. This was what the sugar and cocoa estate owners in Trinidad wanted, with the bonus of being cheap and reliable. Indeed, the Indians who arrived on the Fath al Razack on 30th May 1845 were generally young. With only one exception, all the male emigrants were under age 40.
Health concerns at the Emigration Depot, Garden Reach, Calcutta, India
In India, persons recruited for emigration were subjected to several medical screenings before being allowed into the Emigration depot and on-board ships. These were performed at different points in time by the Civil Surgeon of the District, the Resident Medical Officer at the depot, Bengal’s Medical Inspector of Emigrants, the Protector of Emigrants, the Emigration Agent and the Depot Consulting Surgeon (Laurence, 1994).
The Emigration authorities tried to prevent the spread of epidemic diseases because an outbreak would mean that the group would be detained for a number of days and costs accrued if the ship was waiting. Therefore, from the 1880s the Emigration Agent inspected all the emigrants in the morning and evening, to check for signs of disease, in order to segregate the sick. This was especially done during famine years.
Some of the illnesses treated at the Trinidad Emigration Depot in Calcutta were cholera, dysentery, diarrhoea, fevers, cerebrospinal meningitis, measles, smallpox, respiratory diseases and venereal diseases (Nanhu, 2012).
Health concerns during sea voyages
The first batch of Indentured labourers sailing to Trinidad on the Fath al Razack experienced various health issues as a direct result of the conditions onboard. The mortality rate onboard the ship was high but overall mortality on voyages fluctuated. Bronchitis, diarrhoea, measles, mumps and dysentery were some of the contagious diseases which kept the mortality rate of the immigrants high. An outbreak of cholera also impacted life for the immigrants with exposure to contaminated water onboard.
The mental health of the labourers varied, as a result of the sometimes cold and turbulent weather, as well as the cramped dark spaces with poor ventilation below deck where the Indian labourers were situated in. Some labourers committed suicide by jumping overboard into the rough seas, in the hopes of returning to India, and this heightened the mortality rate onboard the ships (Laurence,1994).
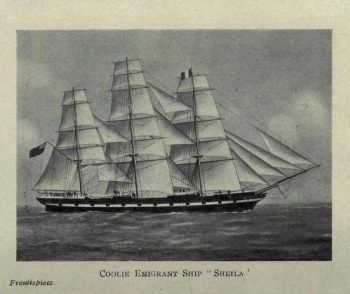
Picture of the Sheila which was used to transport Indentured Indians to Trinidad
Source: Stabroek News
https://www.stabroeknews.com/2017/11/30/features/first-person-singular/the-land-down-under/
Vessels, which transported the Indentured labourers to the colonies after the Fath al Razack experienced similar outbreaks of various diseases, in spite of the numerous medical checks of the emigrants before they left India. The True Briton in 1852 with 313 emigrants suffered 20 deaths; the Hyderabad in the same year with 316 emigrants had 27 deaths. Stomach and bowel disturbances, Asiatic Cholera, and convulsive fits were stated as the causes for the high death rate onboard (Perry, 1969)
As expected, the crew onboard these ships shifted the blame to uncontrollable circumstances and the Indians themselves. On the True Briton, they stated that the torrential weather left them no choice but to close the hatches to discourage leaking on the boat, thereby decreasing ventilation for the already cramped spaces in which the Indians resided. The Hyderabad recruited indentured labourers who already displayed signs of poor health however still proceeded, despite objections from the designated surgeon (Perry, 1969).
Mortality on ships caused concern for planters and governments. In the early phase of the system mortality was mainly the result of the lack of regulations governing the system. Provisions for personal hygiene on emigrant ships were limited so it was a fertile situation for contagious diseases to spread. In the 20th century the chances of survival increased as mortality on voyages declined. The issues on ships included overcrowding, poor quality of food; and a lack of proper hygiene as there were only one or two toilets for all passengers; bad odours or miasma below deck and diseases.
During the 1850s-1860s mortality on voyages to the West Indies rose, especially during the years 1856-58. As a result, the Governor of India set up an enquiry into the mortality rates in 1858. The enquiry found that a major contributing factor to mortality on voyages was the lack of any facility on ships for isolation of sick persons. Other factors contributing to illness included the European doctors’ unfamiliarity with Indian diseases; poor diet, lack of proper sanitation, using contaminated water from the Hooghly river and the mental stress of leaving home and the voyage.
Overall, the mortality on ships fluctuated. For most of the 1850s it was approximately 4%. In 1856-57 there was high mortality of 17.3%. High mortality rates were due to cholera, spread by taking contaminated water on board. The health of emigrants was also a factor—those from districts affected by famine were already weakened and prone to illness. High mortality on ships from Calcutta to the West Indies 1856-57 led to a revision of the rules for emigration. The new rules stipulated guidelines on diet, clothing, medicines, ventilation, cleanliness, hospital records and more (Laurence, 1994).
Each ship had a Surgeon Superintendent who was in charge of the welfare of the passengers. This position was filled by a man, usually recruited in England. He was paid according to how many immigrants landed in the West Indies alive. If neglect or misconduct could be proven on his account, a portion or all of his salary could be withheld (Laurence, 1994).
The Surgeon Superintendent was appointed by the Protector of Emigrants in India. His duties included medical inspection of the Indians, rejection of unfit persons; inspection of the ship and report on ventilation of the vessel. He was also responsible for the arrangements for cooking; setting up a hospital in the deckhouse and checking supplies to put on the ship for the Indians. (Kumar, 2017).
Health issues on arrival in Trinidad
When the Indians arrived in the Caribbean a significant number were usually unwell. They were then sent to the hospital or classified as convalescent or as unfit for immediate labour (Laurence, 1994). Between 1845 and 1866 the Port-of-Spain Harbour was used as a staging area for the receipt, assessment and processing of newly-arrived Indian immigrants. This was called the “Coolie Depot” (Mahase, 2013). Persons who were deemed to be in poor health were sent to the Colonial Hospital while those in good health were given a few days rest before journeying to those plantations which had applied for additional labour months before. However, this system was grossly unpopular with residents and merchants in Port-of-Spain. They complained of worsening vagrancy, poor sanitation and the strain on the Colonial Hospital when an immigrant vessel made port. As a result, the point of arrival for Indian immigrants was permanently moved to the Five Islands in 1866.
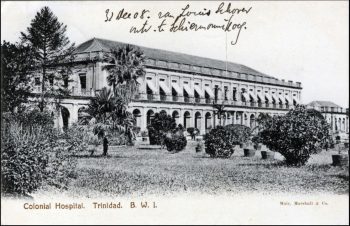
Picture of the Colonial Hospital, Port of Spain, 1908
Source:
https://www.flickr.com/photos/striderv/2481451308
Nelson Island was chosen for the Indian Immigration Depot. Vessels hailing from India docked near Nelson Island and unloaded immigrants onto barges for transfer to the island (Mahase, 2013). Within this period, the islands represented the first contact the immigrants made with Trinidad. Before leaving the vessel, the health of every individual immigrant was assessed by a committee of colonial officials including the Protector of Immigrants, the Medical Inspector of Immigrants, the Harbour Master and the Surgeon Superintendent of the vessel (Tikasingh, 2012).

Picture of Nelson Island Immigration Depot around 1900
Source: The Michael Goldberg Collection, Alma Jordan Library, University of the West Indies
In addition to inspecting the immigrants, the Protector of Immigrants also inspected the ships and reported on the conditions of every vessel and the passengers. The Indians were checked physically; their verification papers were made out and their marriages were registered at the depot (Nanhu, 2012). Their clothes and their ‘jahaji bundles’, i.e. the items that they brought with them wrapped in a cloth, were fumigated. While the authorities used the Nelson Island Immigration Depot for the Indians to recover from the journey for a few days, it was also a way to control the transfer of any contagious diseases brought from India. During this time, a more meticulous medical observation was carried out by the Medical Inspector. Immigrants were then divided into three groups; those physically fit for immediate assignment to the estate, those temporarily unfit for immediate assignment, and those ill enough to warrant their admission to the Colonial Hospital (Tikasingh, 2012).
On Nelson Island, Marion Hospital was used to treat sick Indians. This is significant because no other British colony receiving Indian indentured immigrants had an Immigration Depot set up separately from the mainland. Some of the ailments treated at Marion Hospital included conjunctivitis, ring worm, bronchial catarrh, emphysema, chicken pox, scabies and abortion (Nanhu, 2012). Indians indentured on estates were also sent to Marion Hospital for treatment, depending on the recommendation of the Medical Inspector and approval of the Protector of Immigrants. They were treated at Marion Hospital for one shilling a day (Nanhu, 2012).


The remains of Marion Hospital, where the arriving Indentured Indians were treated on Nelson Island
Photographer: Joseph Bertrand
As the indentureship system grew in both vessel frequency and numbers of immigrants so did the facilities on Nelson Island. Several changes were made. For example, in 1910 a telephone connection to the Head Office in Port of Spain was set up. Additionally, between 1911-1912 lighting at the depot was improved and the Governor approved plans for an Acetylene Plant, which was still relatively new technology at the point in time (Nanhu, 2012). From 1912-1913 a new kitchen was built with a chapatti shed (this was deemed absolutely necessary). There were five barracks capable of housing 1000 people, quarters for the Medical Officer in charge and living facilities for six compounders, a bungalow of five rooms and a gallery for the Protector or Officer-in-Charge, and a hospital for thirty patients (Nanhu, 2012). In addition to this there was an isolation hospital on Lenagan Island, initially built for quarantine situations, but it was also used to care for Indian immigrants who had infectious diseases (DeVerteuil, 2005).
For Indians arriving after a three-month voyage, the stop at the Five Islands was undoubtedly a welcome respite from harsh climatic conditions, strict food and freshwater rations, and the prevalence of diseases such as cholera, typhoid, dysentery and measles (Arora 1981).
Health concerns on estates in Trinidad
On the estates Indians were treated in estate hospitals from 1865. Before 1865 there were no provisions for sick immigrants in Trinidad. They were left to take care of themselves and some became vagrants. In 1866 the Legislative Council of Trinidad stipulated that all estates had to provide hospitals for indentured Indians (Laurence, 1996). However, the estate hospital was not just a place for treatment, it was a part of the plantation system as the overarching aim of the plantation was to get as much labour out of the workers as possible. Hospitals varied across estates in terms of provision of beds, equipment, and staff (Nanhu, 2012). The Indians did not all view the estate hospitals positively. Indeed, many Indians simply walked out of the hospitals at different stages of treatment (Brereton, 2005).
In 1870 the doctors, the official Government Medical Officers, were assigned the role of caring for sick indentured Indians. Trinidad was divided into districts based on wards and each ward was assigned one doctor. However, the doctor to patent ratio was low and while each estate had an assigned doctor, he only visited twice a week. There were several Ordinances from Trinidad’s Legislative Council from 1866 onwards dealing with hospital provisions on estates for indentured Indians (Nanhu, 2012).
The indentured Indians were treated for numerous diseases at the estate hospitals. These included dysentery, malarial fever, rheumatism, anaemia, ankylostomiasis, respiratory diseases, digestive diseases, parasites, skin diseases and malaria. Malaria was the number one disease treated, skin diseases ranked second, third was ankylostomiasis (caused by hookworms) and then digestive diseases and dysentery (Nanhu, 2012).
Trinidad was among several British colonies in the early 20th century where malaria was a serious concern. In Trinidad malaria was prevalent on estates that were low lying and near to swamps in the rainy season. Malaria and ankylostomiasis were both widespread among the Indian indentured population and both diseases weakened their victims. Being physically weak meant that the Indians were prone to other illnesses and infections and it is likely that the Indians contracted both diseases at the same time and repeatedly (Nanhu, 2012). The prevalence of both hookworms and mosquitos were also an indication of the poor sanitation on estates. Despite the high number of cases of diseases and illness treated at the estates’ hospitals, the Immigration Department in Trinidad gave favourable reports on the health of the Indian Immigrants (Nanhu, 2012).
It must be remembered that the changing health provisions for indentured Indians took place in the context of an evolving indentureship system. The provisions were added as recommendations were made from official enquiries and reports and from complaints from the colonies. In Trinidad major changes were introduced regarding health provisions in 1916 (Nanhu, 2012). However, by this time it was relatively late (the system was nearing its end) and only a minority of Indians would benefit. Moreover, medical provisions for Indian indentureship in Trinidad were set in the wider context of medical provisions for the colony, which were already insufficient. The Colonial Government of Trinidad was unable to provide adequate facilities for the entire freed population, and indentured Indians were an addition to this situation. The Indian immigrants however survived and persisted despite the challenging circumstances.
Sources:
Arora, G.S. (1981). Indian Emigration. New Delhi: Puja Publishers.
Brereton, B. (2005). The Experience of Indentureship 1845-1917. In La Guerre and Bissessar, Calcutta to Caroni and the Indian Diaspora, Third Revised Edition.
DeVerteuil, Anthony. (2005). The Western Isles of Trinidad. Port-of-Spain: Paria Publishing.
Kumar, Ashutosh. (2017). Coolies of the Empire: Indentured Indian in the Sugar Colonies, 1830-1920. Cambridge: Cambridge University Press.
Laurence, K.O. (1994). A Question of Labour: Indentured Immigration into Trinidad and British Guiana 1875-1917
Laurence, K.O. (1996). The Development of Medical Services in British Guiana and Trinidad 1841-1873. In Beckles, H. and Shepherd, V. (eds.) Caribbean Freedom: Economy and Society from Emancipation to the Present: A Student Reader, (269-273). London: Hames Curry Publishers, 1996.
Mahase, Radica. (2013). “The Coolie Depot.” YATRA. Port-of-Spain: East Indian Cultural Promotions, May 30.
Nanhu, K. (2012). Health and Medicine during Indian Indentureship In Trinidad 1910 to 1920. (Unpublished MPhil Thesis). University of Oxford.
Perry, John Allen. (1969). A History of the East Indian Indentured Plantation Worker in Trinidad, 1845-1917. LSU Digital Commons.
Tikasingh, Gerad. (2012). Trinidad During the 19th Century: The Indian Experience. Port-of-Spain: East Indian Diaspora.
https://www.stabroeknews.com/2017/11/30/features/first-person-singular/the-land-down-under/
https://www.flickr.com/photos/striderv/2481451308